Chief Dan George playing the role of Old Lodge Skins in the 1970 movie, “Little Big Man.” Whether or not you’ve seen or remember the film, if you’re a practicing therapist, you know the wisdom contained in that quote. No matter how skilled the clinician or devoted the client, “sometimes therapy works, sometimes it doesn’t.”
Evidence from randomized clinical trials indicates that, on average, clinicians achieve a reliable change–that is, a difference not attributable to chance, maturation, or measurement error–with approximately 50% of people treated. For the most effective therapists, it’s about 70%. Said another way, all of us fail between 30-50% of the time.
Of greater concern, however, is the finding that we don’t see the failure coming. Hannan and colleagues (2005) found, for example, that therapists correctly predicted deterioration in only 1 of 550 people treated, despite having been told beforehand the likely percentage of their clients that would worsen and knowing they were participating in a study on the subject!
It’s one thing when “the magic doesn’t work”–nothing is 100%–but it’s an entirely different matter when we go on believing that something is working, when it’s not. Put bluntly, we are a terminally, and forever hopeful group of professionals!
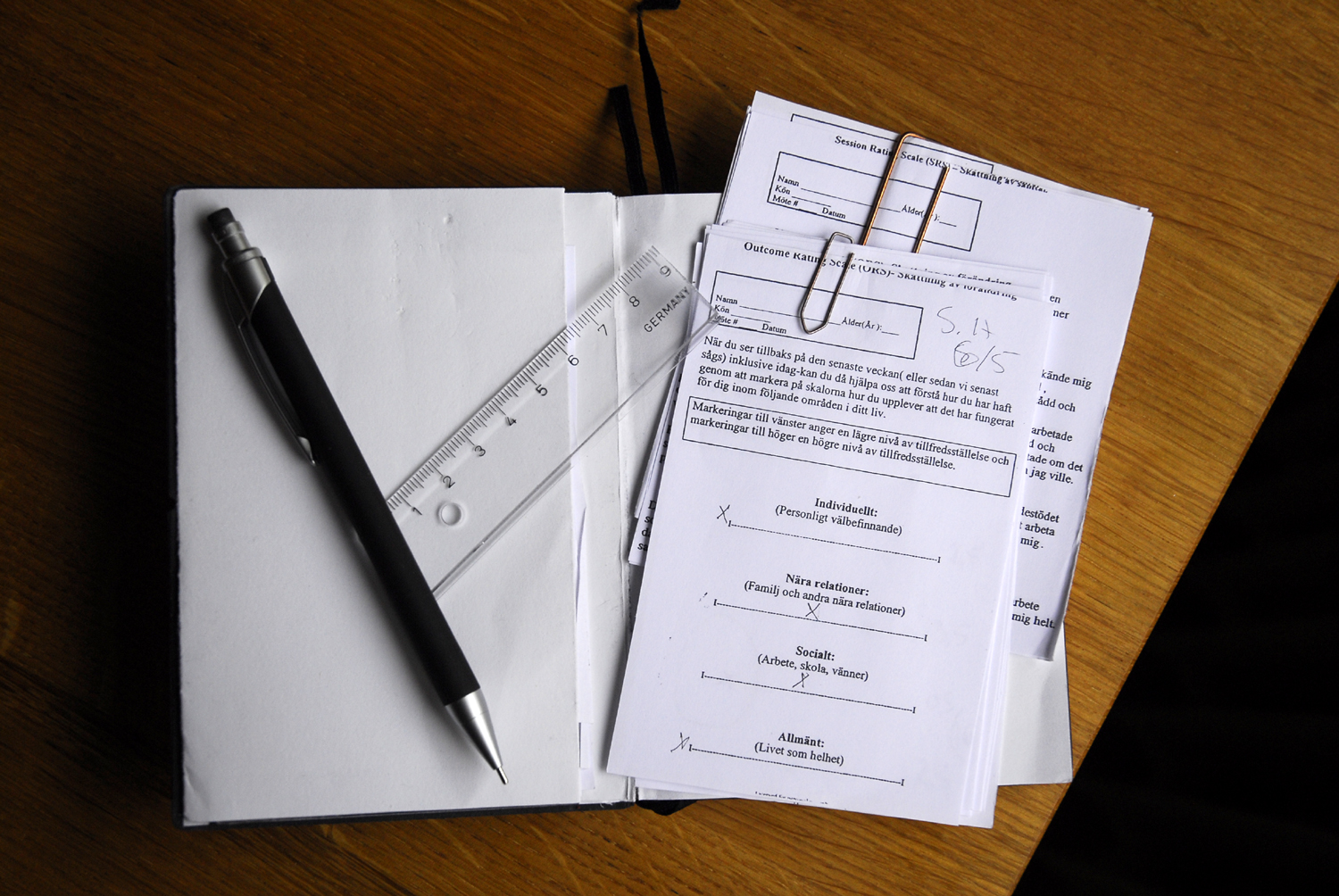
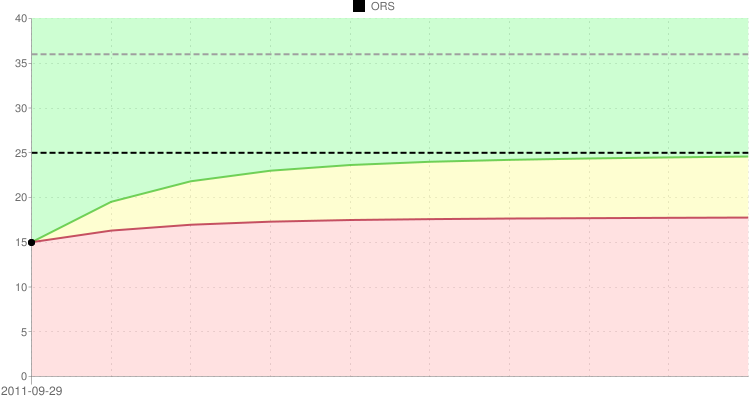
What to do? Hannan et al. (2005) found that simple measures of progress in therapy correctly identified 90% of clients “at risk” for a negative outcome or dropout. Other studies have found that routinely soliciting feedback from people in treatment regarding progress and their experience of the therapeutic relationship as much as doubles effectiveness while simultaneously reducing dropout and deterioration rates.
You can get two, simple, evidence-based measures for free here. Get started by connecting with and learning from colleagues on the world’s largest, online network of clinicians: The International Center for Clinical Excellence. It’s free and signing up takes only a minute or two.
Finally, take advantage of a special offer for the 6 Feedback Informed Treatment and Training Manuals, containing step by step instructions for using the scales to guide and improve the services you offer. These manuals are the reason the ICCE received the perfect scores when SAMHSA reviewed and approved our application for evidence-based status.
Here’s to knowing when our “magic” is working, and when it’s not!

.png)

.jpg)
.jpg)
.jpg)


.jpg)

.jpg)
.jpg)