The evidence shows that using standardized measures to solicit feedback from clients regarding progress and their experience of the working relationship improves retention and outcome.
How much? By 25% (1)
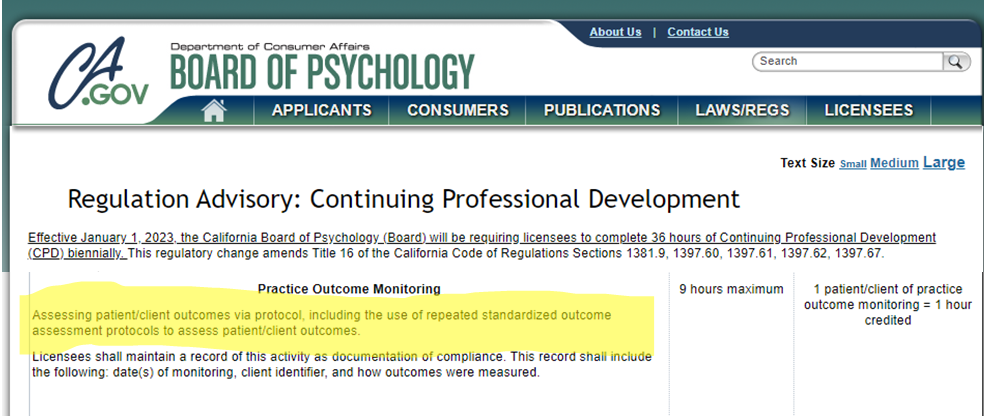
And now, major news out of California.
Psychologists — who are required to earn 36 hours of continuing education credits every other year — can now earn credit towards renewal of their license by implementing feedback-informed treatment (FIT) in their daily clinical work (2)!
Here’s the challenge. The same body of research documenting that FIT works, shows clinicians struggle when it comes to putting it into practice. Private practitioners express concerns about the time it takes. Those working in agencies talk about the challenges of finding alternatives when FIT data indicate the present course of treatment is not working. Finally, many who start, stop after a short while, noting that FIT didn’t add much beyond their “clinical knowledge and experience.”
All such concerns are real. Indeed, as reported a few years back on this blog (3), implemention takes time and skill — in agency settings, up to three years of effort, support and training before the benefits of being feedback-informed begin to materialize. When they do, however, clients are 2.5 times more likely to benefit from care.
So, don’t give-up. Instead, upskill!
In September, the International Center for Clinical Excellence is sponsoring the FIT “Training of Trainers.” Held only once every-other-year, the TOT focuses exclusively on the process of training and supporting others in their use of feedback informed treatment. As with all ICCE events, space is limited to 40 participants. Click on the link above or icon below for more information or to register!
Until next time,
Scott
Scott D. Miller, Ph.D.
Director, ICCE