
 Remember these?
Remember these?
Did you ever own or try one?
Remember Beanie Babies? According to one news story, interest was such, “People neglected other areas of their lives to spend all day trading, and some even invested their children’s college funds in toys that they believed would bring an astronomical return on investment.”
And how about advertising executive Gary Dahl’s product? You remember him, right? In the 1970’s, he became an overnight millionaire selling rocks marketed as pets. Rocks! Waterbeds, Crocs, cause-branded plastic wristbands, oxygen bars, Pogs, Silly Bandz, and the Macarena — the list is as endless as our attention span is short.
If you’ve been in practice for a while, you know the field of mental health is not immune to fad and fashion. Like past diet crazes, the drugs, diagnoses, and treatment methods that capture professional interest and then quickly disappear can be hard to remember. Thus, in the 1980’s it was Xanax, multiple personality disorder, and satanic cult abuse. The 1990’s brought us the “decade of the brain,” borderline personality disorder, and a flood of Prozac and cognitive-behavior therapy knockoffs. More recently, mindfulness, energy meridians, and trauma have become the objets de grand intérêt.
One more trend is Feedback-Informed Treatment (FIT). Known also as Routine Outcome Monitoring, Patient Focused Research, and Measurement-based care, it involves using scales to solicit feedback from clients regarding their experience in treatment and using the resulting information in real time to improve quality and outcome. The weight of the scientific evidence is such that professional and regulatory bodies in the U.S. and abroad have already deemed ROM a “standard” of care in the delivery of psychological services and clinical supervision (American Psychological Association Presidential Task Force on Evidence-based Practice, 2006; Association of State and Provincial Psychology Boards, 2019; Joint Commission, 2018; Tasca et al., 2019).
But is it just another fad?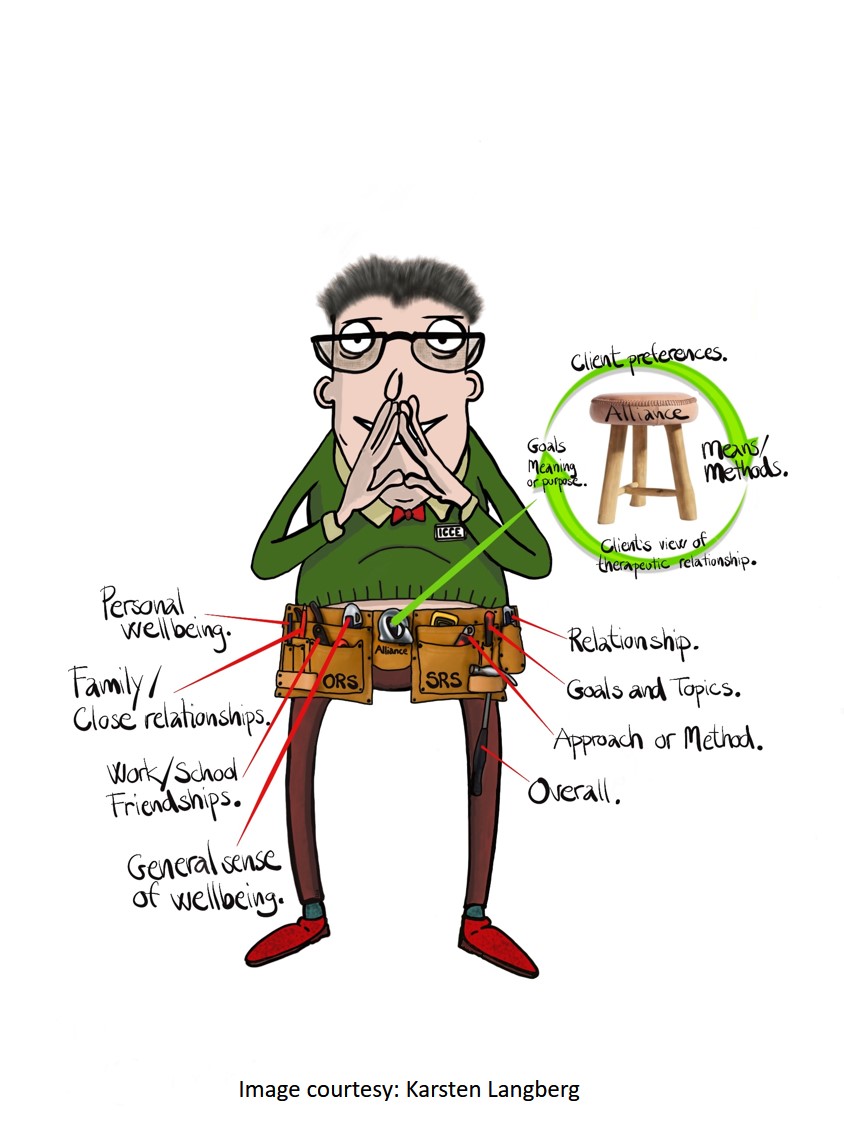
Data from two recent surveys suggest FIT is moving beyond the “innovation” to the “mass adoption” phase among mental health providers and treatment agencies. The study conducted by Myoutcomes® targeted members of Facebook-related psychotherapy interest groups and other sources, finding fairly dramatic growth in: (1) awareness of the empirical support for using measures to assess progress and the quality of the therapeutic relationship; and (2) experience with standardized measurement tools in psychotherapy.
Whether such results indicate FIT will stick around long enough to be the “game changer” remains to be seen. What is known for sure is that, while important, awareness of, experience with, and research support for the process are insufficient to sustain the interest. Research shows, for instance, successful implementation of FIT takes significant time, planning, and support, without which between 70 and 95% of efforts fail. Why? Because working feedback-informed is about changing culture, not using measurement scales in treatment. Success requires that all members of management — from administration to clinical supervisors — understand and are actively involved in implementation. Indeed, when practitioners rather than a team led by a manager are held accountable, the likelihood of FIT being a game changer plummets (80% versus 14 %).
Bottom line? PLEASE don’t download the ORS and SRS and begin experimenting — testing it out to see “if it works.” As I blogged about last week, the likelihood of failure is simply too high. Instead, bring your team to our upcoming Spring intensives in Chicago. You’ll not only “rub shoulders” with colleagues from around the world and our international faculty, but also leave with a thorough grounding in FIT, as well as skills for transforming the culture in which you work.
Until next time,
Scott


Leave a Reply