Do you get those letters about the top healthcare providers in your area?
At the beginning of the new year, our city’s local magazine publishes a list of the top healthcare providers. It’s a big deal. Organized by location and specialty, the issue contains full-page photos, glossy spreads, and breezy write-ups. Impressive stuff with a wide and hungry readership anxious to sort the best from the rest.
So, how do the publishers separate the proverbial “wheat from the chaff?” The answer, depending on whether you are a provider or potential patient, may alternately surprise or frighten you.
Not long ago, Abigail Zuger received one of those letters. In it, she learned that a relative of hers had been named “one of the worlds top physicians in his area of expertise.” Ordinarily, she would have been proud. There was only one problem. Her now esteemed relative was dead–and not just recently. He’d been dead 16 years!
Abigal Zuger is a physician and professor of medicine at Columbia University. The story about her experience appeared in the New York Times. In it, she notes the temptation to become cynical, to dismiss the Top Doc lists, “as just so much advertisement and avarice.” She concludes, however, that a “more nuanced and charitable view is…[that] these services may simply be trying, valiantly if not clumsily, to remedy the single biggest mystery in all of health care…what makes a top doctor…[and] how to find one.”
Three methods dominate among list makers: (1) culling names and addresses from phone directories; (2) polling healthcare providers; and (3) collating patient online ratings. Said another way, consulting available lists lets you know if your healthcare provider once had a phone, was liked by their colleagues, or managed not to piss off too many of the people they treated!
Remarkably absent from the criteria used to identify top providers is any valid and reliable measure of their effectiveness!
Determining one’s effectiveness as a mental health professional is not as difficult or time consuming as it was not long ago. Whether you work with individuals, groups, or families, in inpatient, residential, or an outpatient setting, a simple set of tools is available for monitoring both the outcome and the quality of the services you provide. The tools take minutes to administer and score and are free.
If you are worried about statistics, don’t be. A variety of electronic solutions exist which not only will administer and score the measures but provide normative comparisons for assessing individual client progress and sophisticated analyses of provider, program, and agency effectiveness levels.
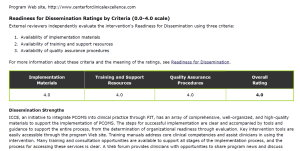
To see what’s possible, check out the Colorado Center for Clinical Excellence. There, clinicians not only measure their effectiveness, but set benchmarks for superior performance and report clinician outcomes transparently on the agency website.