In 2015, colleagues and I released the largest, longitudinal study of therapist effectiveness ever published. The study examined outcomes of 6500 clients treated by 170 practitioners whose results had been tracked an average of 5 years—some as long as 17 years!
The result? Clinician outcomes, on average, not only did not improve, but actually slowly and inexorably worsened with time and experience—and this, despite the fact that practitioners involved in the study routinely measured and had access to ongoing feedback about their results. As I’ve blogged about previously, despite the many claims, measurement and feedback are not enough to improve therapist outcomes.
So, what does work?
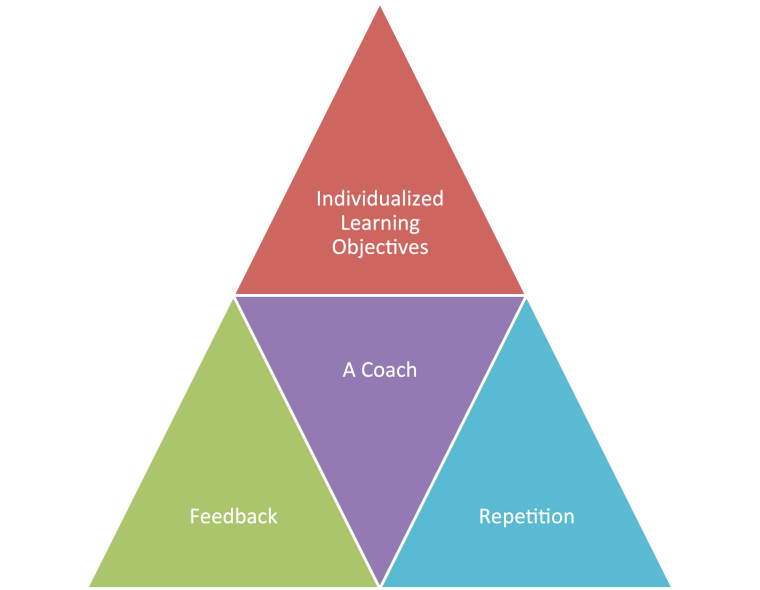 For the last several years, I’ve been advocating deliberate practice (DP)—conscious and purposeful effort aimed at improving specific aspects of an individual’s performance. DP contains four essential ingredients:
For the last several years, I’ve been advocating deliberate practice (DP)—conscious and purposeful effort aimed at improving specific aspects of an individual’s performance. DP contains four essential ingredients:
In short, those wishing to improve must: (1) identify objectives just beyond their current ability and then (2), together with a coach, develop and execute a plan complete with steps and strategies for reaching those performance objectives; (3) throughout, attention must be paid to small errors and mistakes and immediate, corrective feedback provided; finally, (4) with time and repetition, slow but steady improvement results.
To date, research shows time spent in deliberate practice is associated with top performance across a variety of domains, including music, medicine, sports, mathematics, and chess.
With regard to psychotherapy, Chow, Miller et al. (2015) found the most effective clinicians spend more than twice as much time in activities specifically designed to improve their outcomes than their more average counterparts (see Figure 1). The impact of making small but consistent investments of time to deliberate practice is especially dramatic, compounding like interest in a savings account, when results are plotted over time (see Figure 2).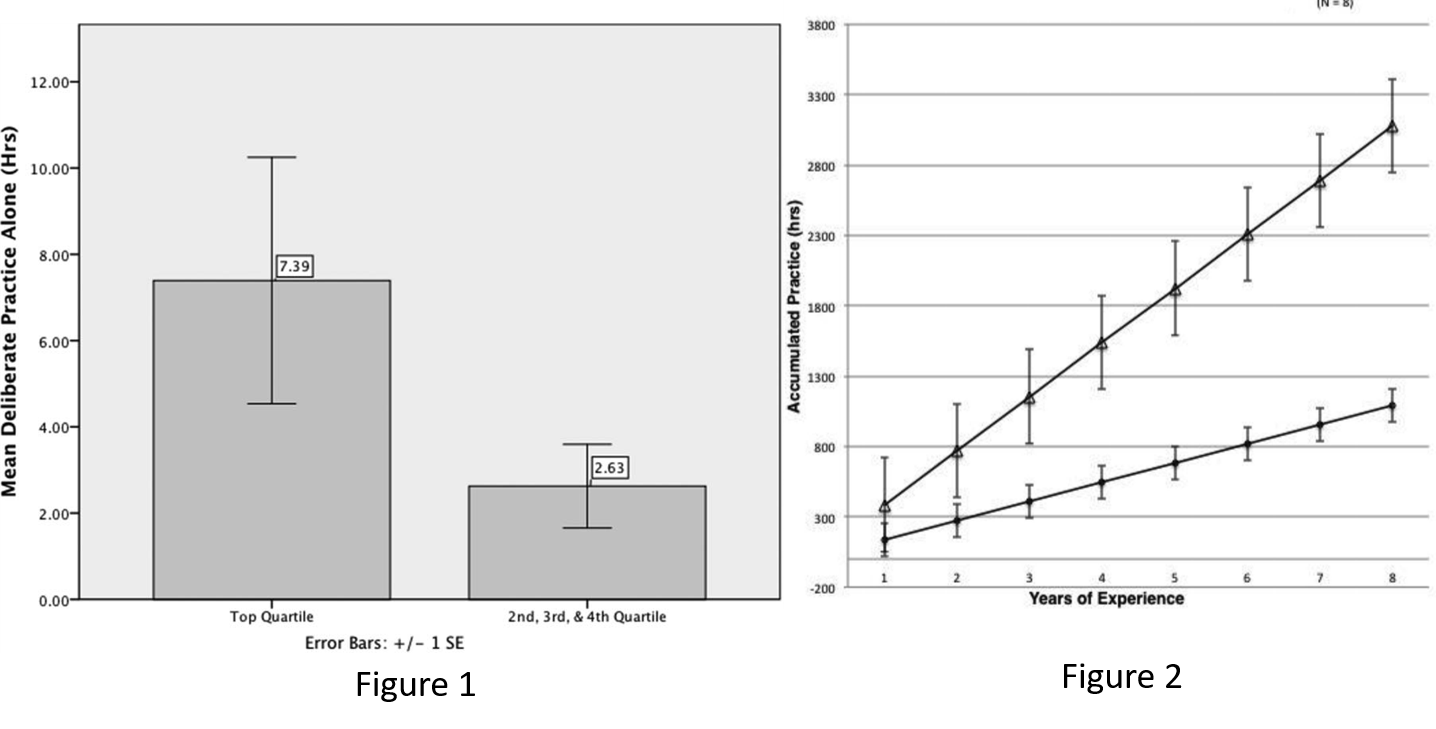
Most important, however, is that the benefit of engaging in deliberate practice extends far beyond mere “statistical significance.” Clients of top performing clinicians, for example, experience 50% more improvement and 50% less deterioration and drop out.
However, as Mark Hubble and I wrote in the “Road to Mastery,” back in 2011, “knowing the facts and putting them into practice are two altogether different matters.” It turns out there’s a reason why most do not devote much time to deliberate practice: it’s hard. Damn hard. Not only is it labor intensive, the rather glacial progress one makes along the way can be pretty discouraging. The key to long term success, it turns out, is community–a complex, interlocking network of people, places, resources, and circumstances working “behind the scenes” to nurture and support ongoing efforts to improve.
And now the data: a study involving more than 150 clinicians and 5500 clients documents what’s possible when agencies work purposefully to create a climate for therapist improvement–specifically, putting systems in place that support deliberate practice in the workplace.
The results? Instead of worsening over time, therapists improved in effectiveness year after year over a seven year period. No, the change in outcome wasn’t dramatic. Rather, consistent with findings in other performance domains, it was slow and stead,y ultimately leading to a large cumulative effect.
What’s it take to get started? The first step is establishing your baseline level of effectiveness. All you need to do to get started is download two, brief measurement tools. Next, get inspired by watching the interview below. Iain Caldwell, the director of an award-winning mental health agency in the U.K, discusses how to develop and sustain a practice committed to superior outcomes and documented professional development. Along the way, we discuss recently published research on the results of a massive government investment in mental health services as well as reports that as many as half of practitioners working within the National Health Service are depressed. Provocative and interesting stuff.