
.jpg)
Some teach. Some write. Some publish research. Arnold Woodruff and Kathy Levenston work for a living! Kathy Levenston specializes in working with foster and adopted children.
Arnold Woodruff developed the first intensive in-home program run by a community services board in Virginia. He has over 30 years of experience, and has served as the President of the Virginia Association for Marriage and Family Therapy. And now, these two dedicated professionals, certified trainers and associates of the International Center for Clinical Excellence, have just purchased Home for Good, the first home-based mental health program in the Richmond, VA area to use Feedback-Informed Treatment (FIT).
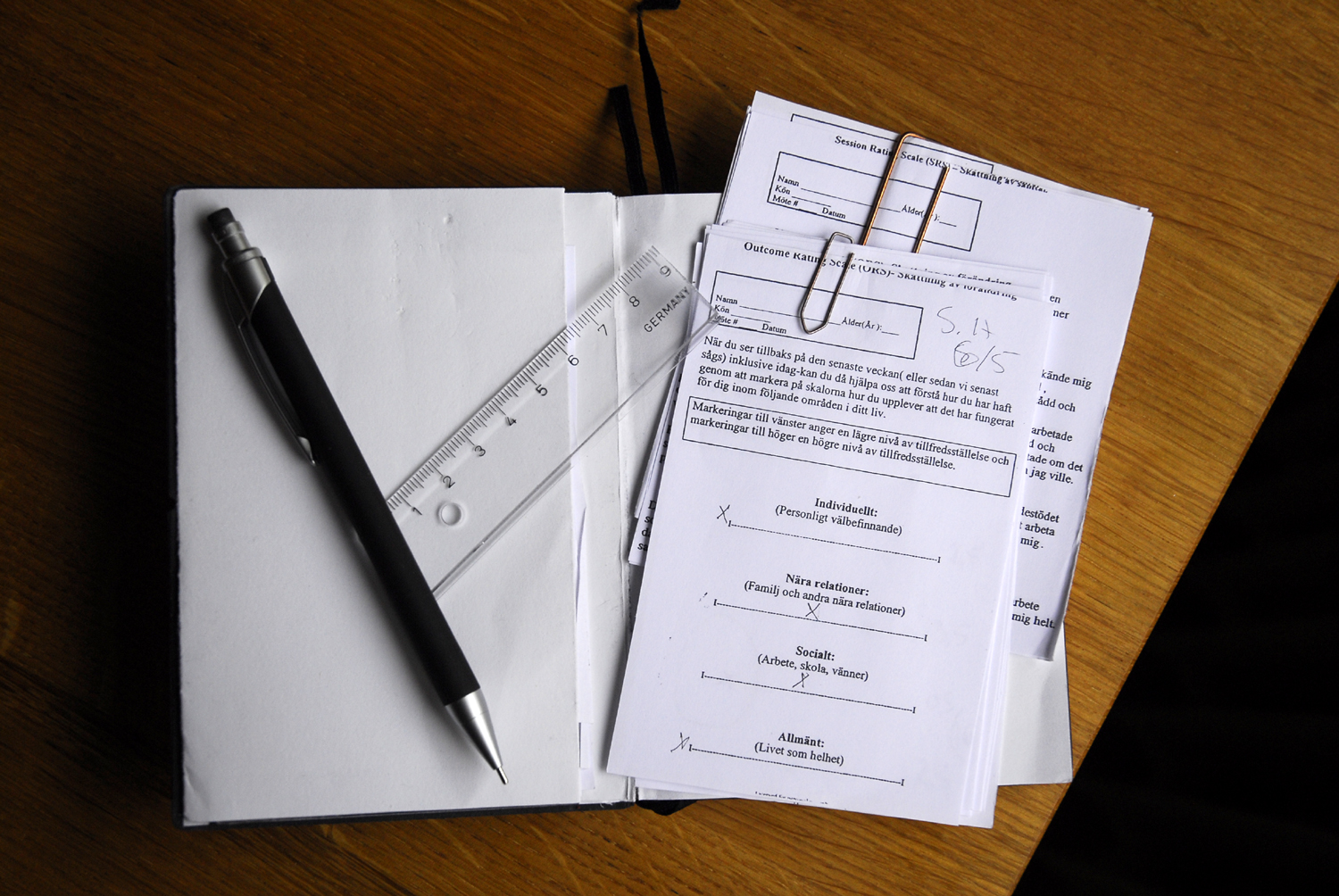
The program is now a 100% employee-owned company and part of a larger vision the two have for establishing customer-friendly mental health care to people in the Richmond area. Home for Good has been providing Intensive In-home Services (counseling, case management, and crisis support) to children, adolescents, and their families for the past two years. Home for Good has achieved superior results compared to other mental health programs, based on an analysis of data genderated from routine administration of the Outcome Rating Scale in clinical practice. Home for Good’s results are continuing to improve with the use of Feedback-Informed Treatment. Home for Good will soon be offering additional services, including outpatient individual, family, and group therapy.
.jpg)


.jpg)
.jpg)







.jpg)
.jpg)




.png)




.gif)




.jpg)
.jpg)

.jpg)



.jpg)

